




















Cardiovascular conditions such as congestive heart failure (CHF) or severe arrhythmias

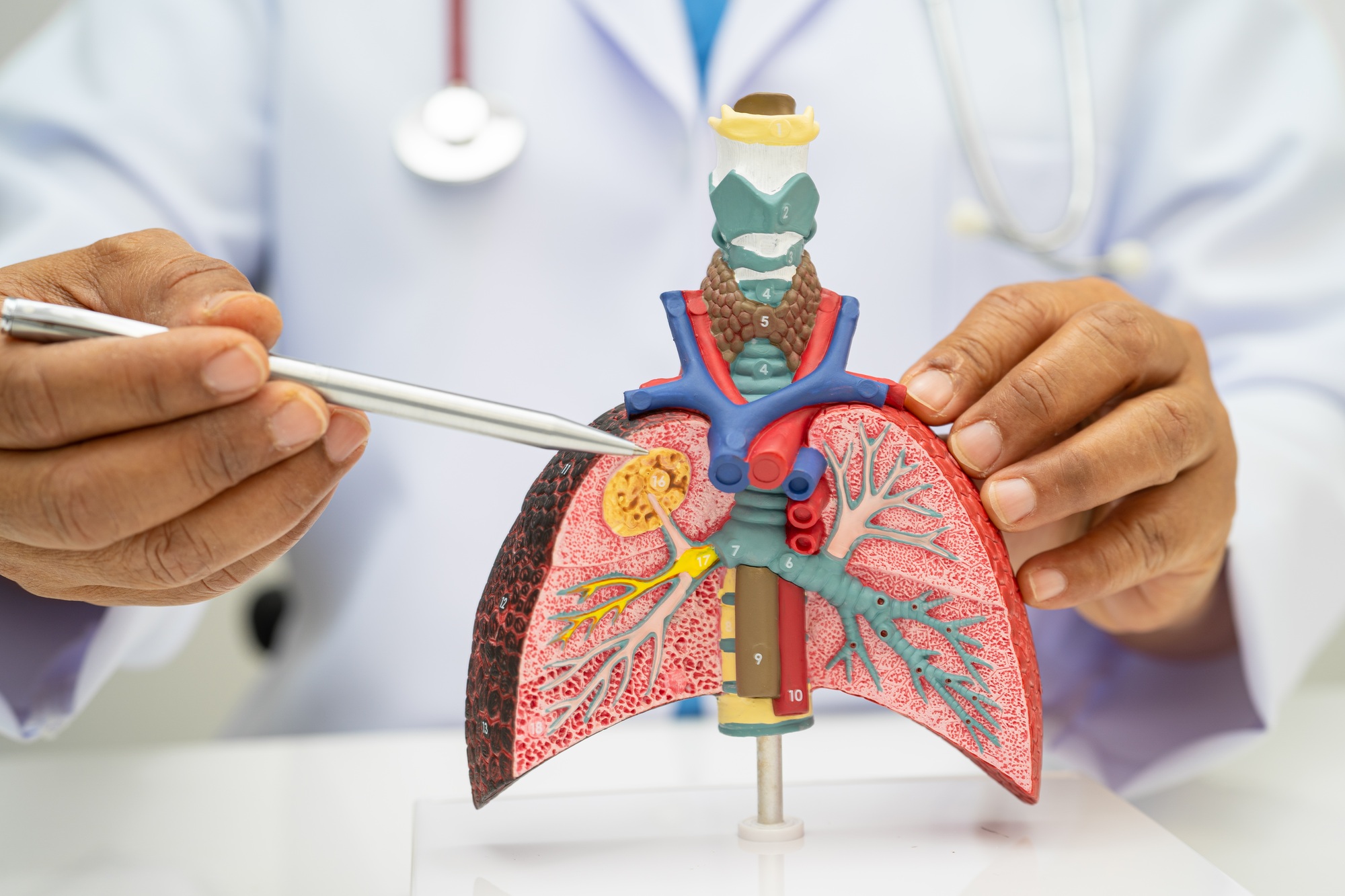
Chronic obstructive pulmonary disease (COPD) or emphysema

Pulmonary fibrosis or other restrictive lung diseases

Neurological disorders that impair respiratory function, such as ALS or other motor neuron diseases




Chronic kidney disease or dialysis dependence

Severe coronary artery disease
Diabetes mellitus with poor control
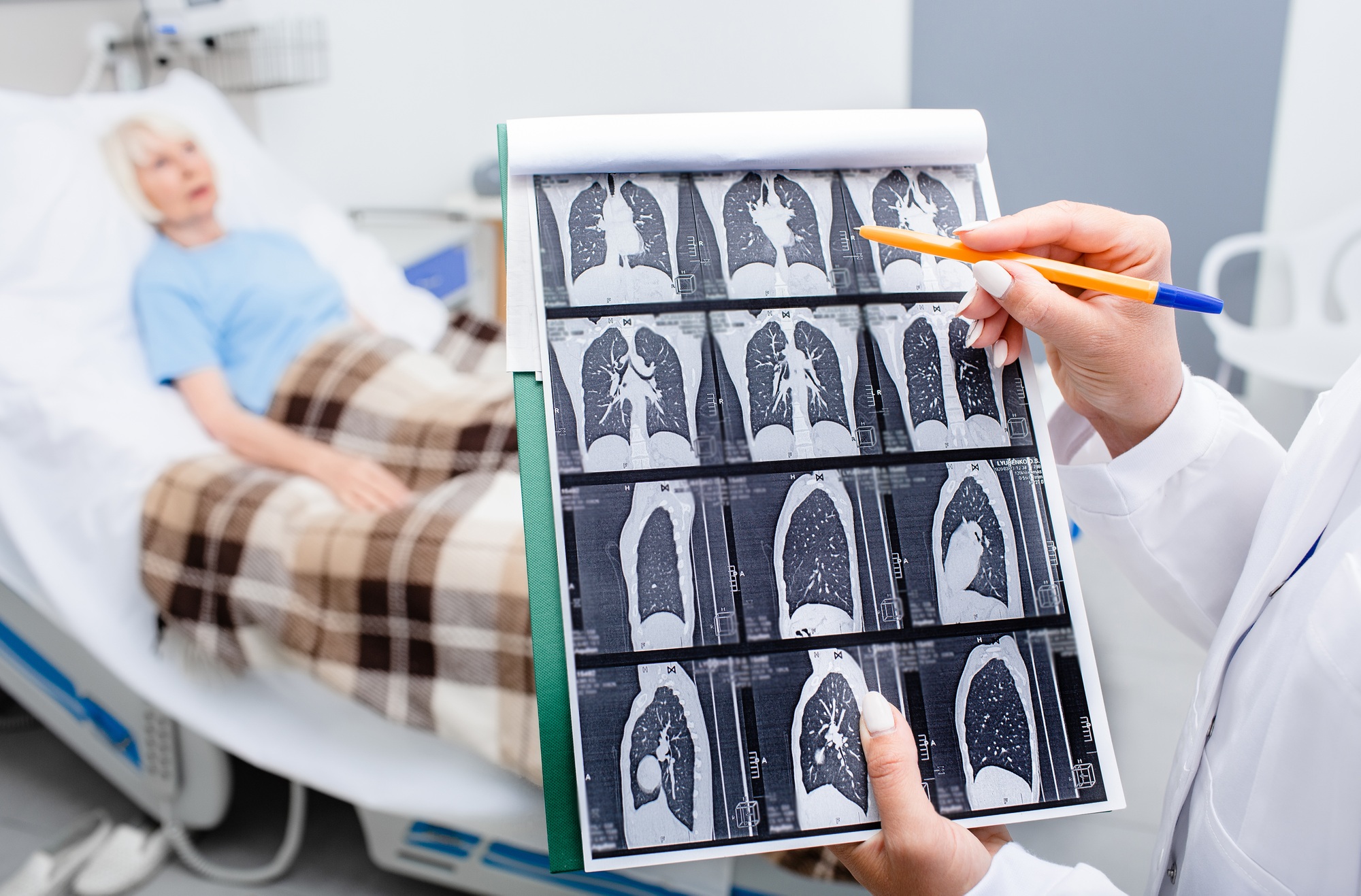
Chronic lung disease such as COPD

Stroke or transient ischemic attack (TIA)

Advanced cancer or other life-limiting comorbidities




Renal insufficiency or dialysis dependence.
COPD or other chronic lung disease.

Diabetes mellitus with end‑organ damage.

Coronary artery disease refractory to revascularization.




Active alcoholism (>80 g ethanol/day)

Hepatocellular carcinoma

Hepatitis B or C refractory to therapy
Post–liver transplant (if awaiting transplant, hospice discharge upon organ availability)



Advanced cardiac or pulmonary disease

Immunosuppression/AIDS
Malignancy



Hyperparathyroidism

Nephrogenic systemic fibrosis

Vascular diseases (e.g., calciphylaxis)




Cardiac disease or pulmonary disease

Renal insufficiency

Neurologic decline (e.g., dementia or Alzheimer's progression)




Traumatic brain injury

Hypoxic-ischemic encephalopathy

Neurological deterioration from another underlying condition




Neurological decline (e.g., HIV encephalopathy, dementia)

Cancer (Kaposi's Sarcoma, lymphoma)

Severe opportunistic infections

Severe coagulopathy or thrombocytopenia




End-stage organ failure (cardiac, pulmonary, renal)

Chemotherapy side effects (bone marrow suppression, neutropenia)

Inability to maintain weight or fluids
